🩺 A Heart-to-Heart About Constipation: When Your Body’s Flow Gets Stuck
Hey, I know it’s late, but I’m glad you reached out.
Look, you don’t need to feel embarrassed talking about this. What you’re describing—the discomfort, the bloating, the feeling that nothing is moving—it’s incredibly frustrating. It’s also one of the most common things I deal with as a doctor. It’s often silent, rarely serious, but it absolutely ruins your quality of life.
I want you to take a deep breath. We’re going to talk about constipation like the completely normal, fixable medical issue that it is. I’m going to explain exactly what’s happening inside your gut, why it happens, and the simple, effective ways we can get things flowing smoothly again. I won’t use complicated language, just honesty and clarity. We’re in this together.
What Constipation Really Is: The Traffic Jam Analogy
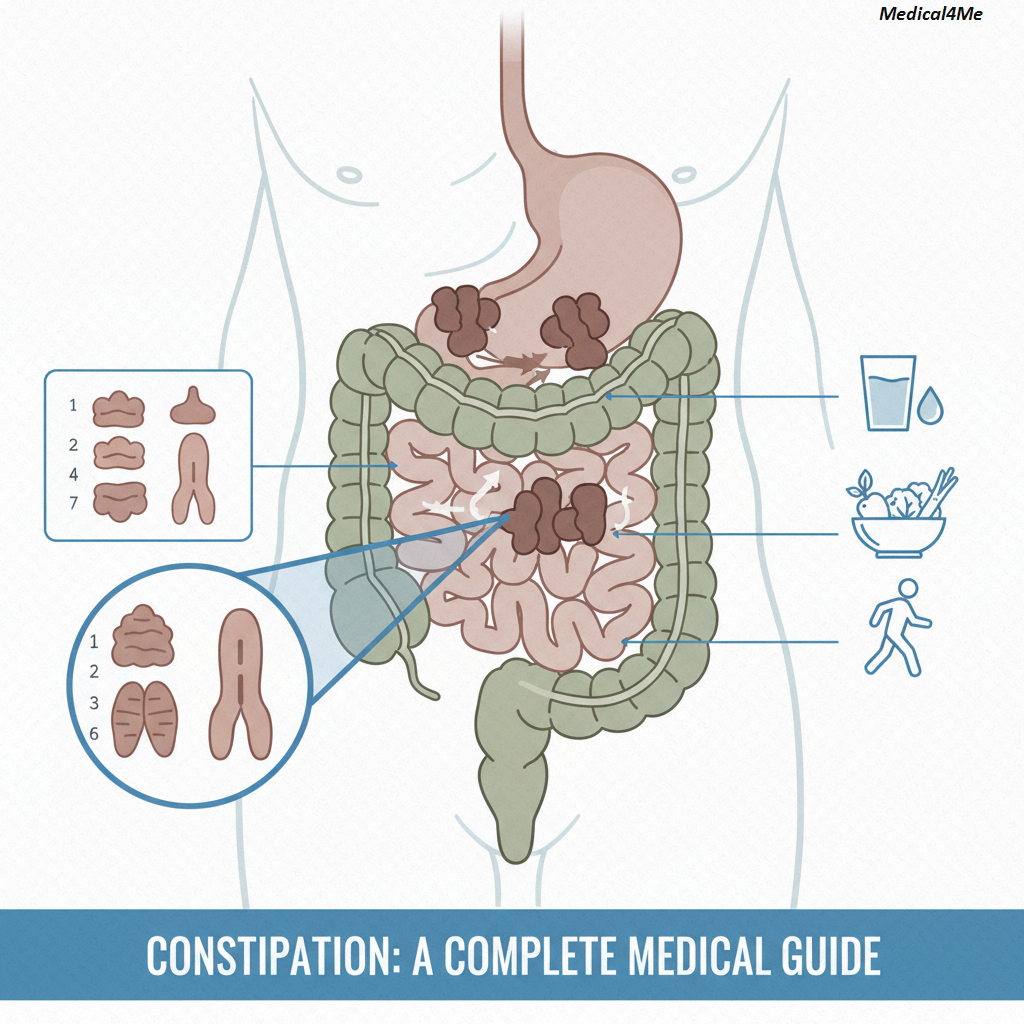
Think of your digestive system as a major highway running through a busy city. Normally, traffic (your food and waste) moves smoothly and quickly from the entrance (your mouth) to the exit.
Constipation isn’t just about how often you go; it’s about the quality of the journey. When you have constipation, it’s like a massive, sudden traffic jam has developed deep inside the highway. There’s a bottleneck. The vehicles start backing up, the pressure builds, and the cargo (the waste) sits there for too long. Because of this delay, the body keeps pulling water out of the backed-up waste, making it harder, drier, and even more difficult to move. This is why the stool becomes hard, small, and painful to pass.
Technically, we define it as having fewer than three bowel movements per week, or experiencing difficulty passing stool that often requires significant straining. But honestly, I define it based on how you feel. If you feel miserable, that’s what we need to address.
The Baffling Slowdown
I remember Ayesha, a wonderful 38-year-old accountant. She was meticulous, managing multi-million dollar books, but her own internal schedule was a mess. She’d always been healthy, running marathons, eating well. But suddenly, she was dealing with severe constipation that came out of nowhere.
She thought she must have a serious disease. However, after listening to her, I realized her job had recently shifted, forcing her to be tied to her desk for 10-12 hours a day. She’d replaced her lunchtime run with desk-side emails. Furthermore, she’d cut back on water because she didn’t want bathroom breaks to interrupt her flow state.
The takeaway? Her highway was physically congested. When we reintroduced her daily exercise and insisted on two liters of water a day, her gut started moving like clockwork again within two weeks. Sometimes, the fix is literally that simple.
Recognizing the Symptoms: When to Pay Attention
It’s completely normal to have an off-day, but when several of these factors persist, they’re red flags. My first thought when a patient describes this is always: Is this a symptom of an underlying issue, or is it purely diet/lifestyle related?
Here are the most common signs you might be dealing with chronic constipation:
- Infrequent Bowel Movements: You’re passing stool less than three times in a typical week.
- Straining and Difficulty: You often have to push or strain during a bowel movement. This shouldn’t be happening.
- Hard or Lumpy Stools: The stool looks like small pellets or rocks (Type 1 or 2 on the Bristol Stool Chart).
- Feeling of Incomplete Emptying: Even after a bowel movement, you feel like you still need to go. This is a telltale sign.
- Abdominal Bloating and Pain: Persistent discomfort or swelling in your stomach area.
- The Need for Assistance: Regularly needing to use your finger to manually assist the passing of stool.
If these signs are new or worsening, it’s time to seek proper care. It’s a completely common reason why people end up talking to a professional here at Medical4Me.
Root Causes: Why the Traffic Jam Starts
To be perfectly honest, the medical community is still exploring the precise mechanism for some forms of functional constipation. However, 90% of cases boil down to a few core problems. We call these the “three major P’s”: Poor Habits, Physical Blockages, and Primary Conditions.
Physical Causes: The Engine Stops
These are the most common things I see causing the gut to slow down:
- Inadequate Fiber Intake: This is like removing the oil from your car’s engine. Fiber adds bulk and water, making the stool soft and easy to push. If you’re eating a lot of processed foods, you’re starving your colon of what it needs.
- Dehydration: As I mentioned in recent posts, your colon’s job is to reabsorb water. If you don’t drink enough, it will pull every drop it can from your stool, turning it into cement.
- Ignoring the Urge: This is often the case with kids or people in demanding jobs. If you habitually ignore the signal to go, your body eventually stops sending the signal, and the stool hardens.
Secondary Causes: The Systemic Slowdown
Sometimes, the constipation isn’t the problem itself; it’s a symptom of something bigger.
- Medications: Many common drugs slow down the gut. This includes certain pain medications (opioids), antacids containing calcium or aluminum, iron supplements, and some antidepressants.
- Underlying Diseases: Conditions that affect metabolism or nerves can slow the entire system. For instance, hypothyroidism (underactive thyroid) is a major culprit because it literally slows the body’s processes down. Also, diseases like diabetes and Parkinson’s can damage the nerves that communicate with the colon.
- Pregnancy: Hormonal changes (progesterone, especially) and the physical pressure of the growing uterus put a big brake on the entire system.
A Diagnosis of Slow Transit
Haroon was 67, a retired civil engineer, and deeply concerned. He’d lived a disciplined life, ate plenty of vegetables, and walked every day. He felt frustrated because none of the simple fixes worked. He said he hadn’t felt relief in six months.
Because of this baffling pattern, we conducted more detailed tests. Haroon was eventually diagnosed with slow transit constipation, a motility disorder where the muscles in the colon just don’t contract strongly enough to move the waste efficiently.
Therefore, his treatment wasn’t about more water or fiber; it was about specific motility-enhancing medications. It taught me again that you can do everything right and still need a deeper medical intervention.
The Diagnostic Journey: Finding Your Specific Cause
When you come to me with symptoms of constipation, my goal isn’t just to prescribe a laxative; it’s to rule out anything serious and pinpoint the exact underlying cause.
The diagnostic journey is step-by-step, thorough, and highly personalized.
- Comprehensive History and Physical Exam: We start by talking. I’ll ask about your diet, medication history, how often you go, and what your stools look like. I’ll also perform a physical exam, which might include a digital rectal exam to check for blockages, painful fissures, or weakened pelvic floor muscles.
- Blood Work to Rule Out Systemic Issues: We’ll do routine blood tests. For instance, we’ll check your thyroid hormone levels (TSH) to rule out hypothyroidism, and we’ll check your calcium levels because high calcium can also cause problems.
- Colorectal Cancer Screening: In older patients (generally over 45-50) or those with other concerning symptoms (like rectal bleeding or unexplained weight loss), we must rule out colon cancer as a cause. This usually means a colonoscopy.
- Specialized Testing (If Needed): If the initial steps don’t reveal the cause and the constipation persists despite lifestyle changes, we might need to assess the mechanics of your colon. This includes tests like Colonic Transit Study (where you swallow tiny markers and we track their movement over several days) or Anorectal Manometry (which assesses the strength and coordination of your anal sphincter and pelvic floor muscles).
Mayo Clinic explains the importance of these mechanical tests when common treatments fail, ensuring we find the right solution for you.
The Treatment Reality: Getting Things Moving Again
The good news is that most cases of constipation are solved with a two-pronged attack: lifestyle adjustments and simple medical help.
Lifestyle: Building a Better Routine
This is the cornerstone of constipation management. This isn’t just about what you eat; it’s about how you live.
- Fiber, Fiber, Fiber: Aim for 25–38 grams of fiber daily. Focus on whole grains, fruits with the skin on, and legumes. You can also use bulk-forming supplements like psyllium (Metamucil) or methylcellulose (Citrucel).
- Hydration is Non-Negotiable: Drink water! Period. I generally advise patients to aim for at least six to eight glasses (about 2 liters) of non-caffeinated, non-alcoholic fluid daily.
- Move Your Body: Physical activity, even a brisk walk, increases blood flow throughout your body, including your gastrointestinal tract. Exercise literally stimulates your gut muscles.
- The Toilet Routine: Try to go at the same time every day, ideally about 30 minutes after breakfast, when the gastrocolic reflex is strongest. Also, consider elevating your knees with a small stool while on the toilet. This changes the angle and straightens the colon, making passing much easier.
Medical Options: Gently Nudging the System
When lifestyle changes aren’t enough, we turn to medications. The goal is gentle, reliable relief, like with other conditions.
Common Medical Treatments for Constipation
The most common medications fall into a few categories:
- Osmotic Agents (e.g., Polyethylene Glycol – Miralax):
- Mechanism: These are non-absorbable substances that draw water into the colon. This makes the stool softer and easier to pass. They are often considered safe for long-term use.
- Side Effects: Bloating, gas, and mild abdominal cramps.
- Stimulant Laxatives (e.g., Bisacodyl – Dulcolax, Senna):
- Mechanism: These work more aggressively. They cause the muscles in the intestine wall to contract (peristalsis), forcefully pushing the stool forward.
- Side Effects: Severe cramping, nausea, and potential for dependency if used excessively. We generally save these for short-term use.
- Chloride Channel Activators (e.g., Lubiprostone – Amitiza):
- Mechanism: These are prescription-strength drugs. They increase fluid secretion in the small intestine, which speeds up movement and softens stool. They’re often used for chronic constipation that hasn’t responded to over-the-counter options.
- Side Effects: Nausea, diarrhea, and abdominal pain.
Comparing Common Laxatives
| Feature | Bulk-Forming (Fiber Supplements) | Osmotic Agents (PEG/Lactulose) |
|---|---|---|
| Pros | Most natural, safe for long-term use, improves overall gut health. | Very effective, gentle action, low risk of dependency. |
| Cons | Requires plenty of water, can cause significant initial gas and bloating. | Can cause dehydration if not used with enough water, prescription options are expensive. |
| Speed | 2–3 days for full effect | 12–72 hours |
The Burden of Medications
Zara, a vibrant 52-year-old grandmother and part-time nurse, came to see me because her constipation was unbearable. She had recently had a shoulder injury and was taking an opioid painkiller (oxycodone). The opioid was a lifesaver for her pain, but it completely paralyzed her gut. She hadn’t gone in days.
We can’t just stop the pain medication, so we had to manage the side effect. We immediately prescribed an osmotic laxative (Miralax) combined with a gentle stimulant (Senna) for a few days to clear the current blockage. The biggest lesson for Zara was understanding the drug interaction. Now, whenever she has to take strong pain medication, she automatically starts the gentle laxative regimen, proactively managing the expected constipation. It’s all about foresight.
When Constipation is a Warning Sign
While constipation is usually manageable, there are certain signs that suggest you need to be seen immediately, as they could indicate a serious or even life-threatening condition.
I want you to be aware of these specific red flags:
- Blood in Stool: Any visible blood, whether bright red or dark and tarry. This needs immediate investigation to rule out conditions like fissures, polyps, or cancer.
- Unexplained Weight Loss: Losing weight without trying, especially when accompanied by changes in bowel habits.
- Severe, Persistent Abdominal Pain: Pain that is crippling or relentless, rather than just mild discomfort.
- Inability to Pass Gas (Flatulence): This suggests a possible bowel obstruction (a physical blockage) and is a medical emergency.
- Vomiting: Especially if it occurs with the inability to pass gas or stool, indicating a serious blockage in the upper digestive tract.
If you experience any of these, don’t wait. We need to assess you right away to ensure your health and safety.
Common Questions I Get About Constipation
Frequently Asked Questions My Patients Ask
Absolutely. Your gut and brain are intimately connected by the vagus nerve. Stress and anxiety flood your system with hormones that can slow down gut motility, effectively putting the brakes on your digestive system.
It depends entirely on the type. Bulk-forming (fiber) and most osmotic laxatives (like PEG) are generally safe for daily use. However, you should never take stimulant laxatives every day, as your body can become dependent on them.
For many people, yes. Coffee contains acids that can stimulate the release of certain hormones, initiating what’s called the gastrocolic reflex. It’s often used as a mild, natural stimulant for the morning.
There is no single “right” answer. Normal ranges from three times a day to three times a week. The key is consistency and comfort. If you’re consistent and the stool is soft and easy to pass, you’re fine.
Yes, iron is notorious for causing constipation. If you need iron (due to anemia), you must proactively increase your water and fiber intake, and sometimes we need to add a gentle laxative to counteract the effect of the iron.
Yes. Chronic straining can lead to hemorrhoids and anal fissures (tears). Severe, untreated constipation can rarely lead to fecal impaction, requiring manual removal. That’s why CDC guidelines state the importance of prompt management.
No, it’s extremely common, but we treat it gently. We primarily use fiber supplements and osmotic laxatives, as other agents may not be safe for the developing baby. We always prioritize the safest approach for mother and child.
My Final Professional Advice
Look, I know how frustrating and isolating this can feel. You can’t see it, you can’t always control it, and it affects every minute of your day. But I want you to remember Zara, Haroon, and Ayesha. They all found a solution, and so will you.
Your body is resilient, but it needs the right fuel and the right pathway. Start with the basics: water and movement. If those simple changes don’t work after a week, don’t just suffer in silence. Come talk to us. We have safe, effective, and targeted medical tools to get your system back on track.
Don’t let a traffic jam on your internal highway ruin the rest of your day. Take control of this, and feel better soon.

Medically Reviewed By
Dr. Saqlain Mushtaq, MBBS
Lead Medical Author, Medical4Me.com
About Our Editorial Process
💬 Share Your Experience
Share your thoughts, questions, or personal tips below. Our community and editorial team value respectful and insightful discussions.