Coronary Artery Disease
I know why you’re calling so late. The term Coronary Artery Disease (CAD) sounds intimidating, complex, and frightening, especially when a loved one—or even you—receives that diagnosis.
Please, let’s take a deep breath together.
You don’t need to fear the label; you need to understand it. My mission isn’t just to treat the disease, but to empower my patients. Therefore, I want to talk to you tonight, not as a doctor to a patient, but as a friend. I want to clear away the medical jargon and give you the professional, precise information you deserve, but delivered with the warmth of a simple conversation.
Because of this, we’re going to break down what Coronary Artery Disease really is, why it happens, and most importantly, how incredibly manageable and treatable it can be when we work together. There are so many positive steps we can take, and you should feel encouraged, not defeated.
What Coronary Artery Disease Really Is: The Plumbing Analogy
Imagine your heart is the most essential, hard-working pump in a massive, beautiful mansion. It never stops, always working to push fresh water (oxygen-rich blood) to every single room.
Now, even a pump needs its own fuel supply. The heart gets its fuel from three major pipes—the coronary arteries—that wrap around the heart muscle. They’re tiny, but vital.
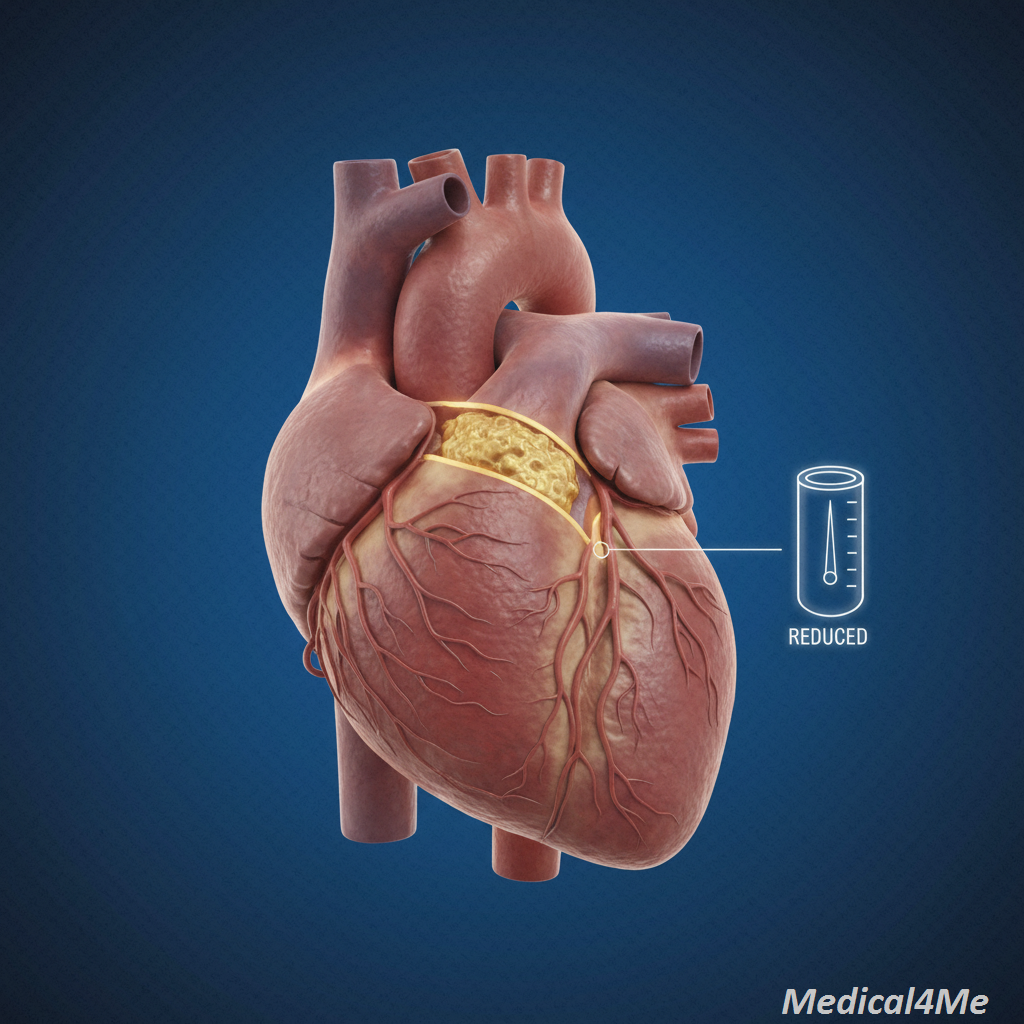
Coronary Artery Disease (CAD) is what happens when those essential pipes get clogged or hardened.
The scientific term for this clogging isatherosclerosis. It’s the slow, frustrating buildup of fatty deposits, cholesterol, and other substances (called plaque) along the inner walls of the arteries. As this plaque hardens, the pipe narrows.
Consequently, when the heart tries to work harder (like during exercise or stress), the narrowed pipes can’t deliver enough blood and oxygen. This lack of oxygen causes the chest pain you hear about, which we call angina. In addition, if a piece of that plaque breaks off and completely plugs the pipe, that’s when a heart attack occurs. It’s a sudden, complete blockage of the fuel line.
Rashid’s Story: The Silent Alarm
I’ll never forget Rashid, a 55-year-old software architect. He came to see me because he was experiencing a baffling, persistent ache in his jaw and left arm when he played tennis. He thought it was a pinched nerve or a strange dental problem. Since he looked fit and was relatively young, he dismissed it.
However, when I heard the symptoms, my internal monologue always shifts immediately to the most serious possibility: Could this pain be referred from the heart? Because of this, we did the tests, and sure enough, he had significant blockages—classic Coronary Artery Disease.
The lesson? Heart pain doesn’t always look like it does in the movies. It can be subtle, manifesting as pain in the back, jaw, or arm. Rashid’s story reminds us that symptoms often appear during exertion because that’s when the heart demands more oxygen than the narrowed arteries can supply.
Recognizing the Symptoms: Listening to Your Heart
The signs of Coronary Artery Disease vary dramatically from person to person. For some, the first sign is a heart attack; for others, it’s decades of subtle discomfort. Recognizing these symptoms is the first step toward reclaiming your health.
Here are the most common ways CAD expresses itself:
- Angina (Chest Pain): This is the most classic symptom. It usually feels like pressure, heaviness, squeezing, or aching in the chest. It often worsens with physical activity and gets better with rest.
- Shortness of Breath (Dyspnea): Feeling unusually breathless, especially after mild exertion or when lying down, suggests your heart muscle isn’t getting enough oxygen to pump efficiently.
- Pain in Other Body Parts: Referred pain in the jaw, neck, throat, upper abdomen, back, or arms (especially the left) can be a sign of the heart struggling.
- Extreme Fatigue: Persistent, unexplained exhaustion that limits your normal daily activities.
- Dizziness or Lightheadedness: Can indicate poor blood flow to the brain, which might be linked to underlying cardiovascular issues.
- Sweating (Diaphoresis): Unexplained cold sweats, particularly when accompanied by chest or arm discomfort.
Root Causes: Why the Plaque Builds Up
The process of atherosclerosis that leads to Coronary Artery Disease isn’t random; it’s a result of a complicated interaction between genetics, inflammation, and lifestyle. To be perfectly honest, the medical community is still exploring the precise mechanism by which the immune system and certain white blood cells contribute to plaque *instability*—the part that causes the heart attack. Nevertheless, the risk factors are crystal clear.
Major Controllable Risk Factors
These are the elements we can actively change, which gives us immense power over the disease:
- High Blood Pressure (Hypertension): Chronically high pressure damages the inner lining of the arteries, creating entry points for plaque formation.
- High Cholesterol (Hypercholesterolemia): Specifically, high levels of LDL (“bad”) cholesterol, which gets deposited into the damaged artery walls.
- Smoking: Tobacco smoke causes immediate damage to the coronary artery linings and raises blood pressure dramatically, accelerating plaque buildup like nothing else.
- Diabetes: High blood sugar levels injure the blood vessels throughout the body, making them stiff and inflamed, severely increasing the risk of CAD.
- Obesity and Sedentary Lifestyle: Lack of regular physical activity contributes directly to poor cholesterol profiles and high blood pressure.
Non-Controllable Risk Factors
- Age: The risk naturally increases as you get older.
- Sex: Men generally have a higher risk than women, but women’s risk increases sharply after menopause.
- Family History: A strong family history of early heart disease is a significant independent risk factor.
The Quiet, Stubborn Risk
I remember Sameer, a 48-year-old school counselor who was incredibly fit. He ran marathons, didn’t smoke, and his diet was impeccable. He couldn’t believe it when his tests showed significant plaque buildup. “I’m doing everything right, Doctor!” he insisted.
Sameer’s issue was almost entirely familial hypercholesterolemia (FH)—a genetic condition. Because of this genetic burden, his liver was simply programmed to produce too much LDL cholesterol, regardless of his lifestyle.
The resolution? We had to treat his cholesterol aggressively with high-intensity medication. His case proves that heart disease isn’t always a “lifestyle failure.” Sometimes, it’s a genetic challenge we have to manage, like with other conditions.
The Diagnostic Journey: Finding Your Heart’s Truth
If I suspect a patient has Coronary Artery Disease, the journey to diagnosis is deliberate, non-invasive where possible, and highly effective.
- Patient History and Risk Assessment: We start with a long conversation about your symptoms, family history, and lifestyle. This tells me about 80% of what I need to know.
- Electrocardiogram (ECG/EKG): This quick, painless test records the electrical signals as they travel through your heart. It can show signs of previous heart attacks or current reduced blood flow.
- Blood Tests: We check cholesterol and triglyceride levels, high-sensitivity C-reactive protein (an inflammation marker), and blood sugar (HbA1c).
- Stress Testing (Exercise or Pharmacological): We monitor your heart while it’s working hard. A treadmill test is standard. If you can’t walk, we use medication to make your heart beat faster, simulating exertion. If the ECG shows changes during stress, it suggests CAD.
- Echocardiogram (Echo): An ultrasound of the heart that shows us the pump function (ejection fraction) and if the heart muscle has been weakened by poor blood flow.
- Coronary Computed Tomography Angiography (CCTA) or Cardiac Catheterization: If the non-invasive tests are highly suggestive of blockages, we move to imaging. CCTA is a non-invasive CT scan to look at the arteries. The most definitive test is Cardiac Catheterization, where a tiny tube is inserted into an artery (usually in the wrist or groin) and guided to the heart to inject dye and get clear pictures of any blockages.
Mayo Clinic explains the importance of starting with the simplest, least-invasive tests first. This phased approach ensures accuracy while keeping you comfortable.
Treatment Reality: A Path to Healing
The wonderful thing about Coronary Artery Disease is that treatment isn’t about resignation; it’s about control and prevention. We aim to halt the plaque growth, manage symptoms, and reduce the risk of future events.
Lifestyle: The Foundation of Recovery
This is the most powerful medicine you have. We can’t bypass this step.
- Dietary Overhaul: I always advise the Mediterranean or DASH diet—rich in fruits, vegetables, whole grains, and lean protein, and low in saturated fats and sodium.
- Regular Exercise: Aim for at least 30 minutes of moderate activity most days. Walking, swimming, or cycling strengthens the heart muscle and improves blood pressure and cholesterol.
- Smoking Cessation: This is non-negotiable. Quitting smoking provides the most immediate, dramatic benefit to your long-term heart health.
- Stress Management: Unmanaged, chronic stress contributes to high blood pressure and inflammation. Practices like deep breathing, meditation, or quiet hobbies here at Medical4Me can make a real difference.
Medical Options: Stabilizing the Arteries
Medication plays a dual role: treating the immediate symptoms and slowing the underlying disease progression.
Common Medical Treatments for Coronary Artery Disease
The most common medications fall into a few categories:
- Antiplatelet Agents (e.g., Aspirin, Clopidogrel – Plavix):
- Mechanism: These drugs prevent blood platelets from clumping together and forming clots, which are the immediate cause of heart attacks. They effectively “thin” the blood.
- Side Effects: Increased risk of bleeding (easy bruising), and rarely, stomach irritation.
- Statins (e.g., Atorvastatin – Lipitor, Rosuvastatin – Crestor):
- Mechanism: These are cholesterol-lowering superheroes. They block an enzyme the liver needs to produce cholesterol, significantly reducing the circulating LDL (“bad”) cholesterol available to form new plaque.
- Side Effects: Muscle aches (myalgia) are the most common complaint, and sometimes liver enzyme elevation.
- Beta-Blockers (e.g., Metoprolol, Atenolol):
- Mechanism: They literally slow the heart rate and reduce blood pressure. This decreases the amount of oxygen the heart muscle needs, relieving angina and protecting the heart from future strain.
- Side Effects: Fatigue, cold hands/feet, and sometimes dizziness.
Invasive Treatments
When blockages are severe or symptoms are uncontrolled, we turn to procedures:
- Percutaneous Coronary Intervention (PCI) / Angioplasty and Stenting: This is a non-surgical procedure where a balloon is inflated inside the blocked artery to push the plaque back, and a mesh tube (stent) is left behind to keep the artery open.
- Coronary Artery Bypass Grafting (CABG): A major surgical procedure used for multiple, widespread, or highly complex blockages. A healthy blood vessel is harvested from another part of the body (like the leg or chest) and used to create a “bypass” around the blocked coronary artery.
Comparing Treatment Options: PCI vs. CABG
| Feature | Percutaneous Coronary Intervention (PCI/Stent) | Coronary Artery Bypass Grafting (CABG) |
|---|---|---|
| Pros | Minimally invasive, shorter hospital stay, quicker return to normal activity. | Excellent long-term results, best for complex disease (multiple vessels, difficult locations). |
| Cons | Higher chance of re-blockage (restenosis), not ideal for certain complex anatomy. | Major surgery, longer hospital stay (5-7 days), 6-12 week recovery period. |
| Use Case | Single or simple blockages, or during an acute heart attack. | Extensive, three-vessel disease, or in patients with diabetes. |

The Necessary Procedure
Usman, a 72-year-old retired truck driver, was managing his stable angina for years with medication. He took his statins and beta-blockers religiously, but recently, his angina started coming back, even with minimal activity. He was terrified.
We performed a cardiac catheterization, which confirmed a very tight 95% blockage in his Left Anterior Descending (LAD) artery—a crucial vessel.
We couldn’t manage that with pills alone.
Consequently, we performed a PCI and placed a stent. Usman was anxious, but the procedure took less than two hours. He was home the next day and, within a week, was walking further than he had in months without any chest pain. It was a clear demonstration that intervention, when necessary, can dramatically and immediately improve quality of life and prognosis.
When to Seek Immediate Help
While some symptoms are chronic and manageable, others signal an emergency. If you or a loved one experiences any of the following, seek emergency medical care immediately. Don’t drive yourself—call the ambulance.
- Sudden, Severe Chest Pain: Pain that is crushing, feels like a tight band, or radiates sharply down the arm or up to the jaw, and oesn’t subside with rest or nitroglycerin (if prescribed).
- Profuse Sweating and Nausea: Chest discomfort accompanied by breaking out in a cold sweat, feeling extremely nauseous, or vomiting.
- Rapidly Worsening Angina: Chest pain that becomes noticeably more frequent, lasts longer, or occurs with less exertion than usual. This is called unstable angina and often precedes a heart attack.
- Unexplained Collapse or Fainting: Sudden loss of consciousness, which may indicate a severe, life-threatening rhythm disturbance.
WHO data shows cardiovascular disease remains the leading global cause of death, emphasizing why recognizing these moments is so critical.
Common Questions I Get About Coronary Artery Disease
Frequently Asked Questions My Patients Ask
While advanced plaque can’t be melted away instantly, aggressive lifestyle changes (especially diet and exercise) and statin use can stabilize the plaque and, in some cases, slightly reduce its volume, significantly decreasing the risk of rupture.
Nitroglycerin is generally taken sublingually (under the tongue) at the onset of angina. If the pain doesn’t go away within five minutes, take a second dose. If it doesn’t go away after the third dose, call emergency services immediately.
Absolutely not. You must continue to exercise! Physical activity strengthens the heart. We just need to tailor the intensity based on your testing (like the stress test) and make sure you understand your safe limits.
No. CAD is the plumbing problem (clogged arteries). Heart failure is the consequence—it means the heart muscle itself has been weakened (often due to years of CAD or heart attacks) and can’t pump blood as efficiently as it should.
Generally, if you can climb two flights of stairs without chest pain or significant shortness of breath, you’re safe to resume intimacy. We usually advise patients to wait a few weeks after a major event and discuss it with us first.
Not at all. Taking medication is a sign of strength and responsibility. If you have a biological or genetic predisposition, medication is the necessary tool to balance the playing field. CDC guidelines state the primary treatment for CAD involves medicine.
Statins can sometimes interfere with enzymes in the muscle cells, causing mild to moderate aches (myalgia). If you feel severe muscle pain, you should definitely tell your doctor right away, as it warrants switching to a different medication.
My Final Professional Advice
I’ve shared a lot of medical science tonight, but I want you to walk away with one simple, powerful feeling: Hope.
Coronary Artery Disease is a serious, chronic condition, yes. But it is entirely manageable. The best outcomes I’ve seen in my practice—like with Rashid, Sameer, and Usman—always involve a patient who takes an active, educated role in their own care. They choose to stop smoking, they choose the salad, and they take their medication.
You have the power to change the trajectory of this disease. Don’t let fear paralyze you. Instead, use this knowledge to guide your actions. Start small. Pick one thing—maybe drinking more water, or taking a 20-minute walk—and commit to it.
The journey to a healthy heart isn’t a race; it’s a marathon. I’ll be here with you every step of the way. Take care.

Medically Reviewed By
Dr. Saqlain Mushtaq, MBBS
Lead Medical Author, Medical4Me.com
About Our Editorial Process
💬 Share Your Experience
Share your thoughts, questions, or personal tips below. Our community and editorial team value respectful and insightful discussions.