Diverticulitis: Symptoms, Causes, and Treatment
I can hear the worry in your voice even though we aren’t in the same room right now. It’s late, the house is quiet, and you’ve probably spent the last hour spiraling down a Google search rabbit hole that made everything seem terrifying. Take a deep breath. Seriously, do it with me right now. I want you to pour yourself a glass of water or a cup of tea, sit down, and just listen. As your friend, and as Dr. Saqlain, I’m going to walk you through this. We’re going to demystify Diverticulitis together, strip away the scary jargon, and look at the facts.
What Diverticulitis Really Is
Let’s start with the basics because understanding the “what” takes away a lot of the fear.
Imagine you have an old bicycle tire. You know how, if the rubber gets a little weak in one spot and you pump it full of air, a little bubble might bulge out from the side? That’s essentially what happens in your colon. These little bubbles or pockets are called diverticula. Having them is incredibly common—like having gray hair as we get older—and that condition is just called diverticulosis.
However, Diverticulitis happens when one of those little tire bubbles gets infected or inflamed. It’s not just a pocket anymore; it’s an angry, red, painful problem.
To be perfectly honest, the medical community is still exploring the precise mechanism of why this infection triggers in some people and not others. For years we blamed popcorn and nuts, thinking they got stuck in the pockets, but we now know that’s mostly a myth.
My first thought when a patient describes that specific, sharp pain in their side is always, “Okay, we need to see if the tire is just bulging, or if it’s about to pop.” It’s a crude way to put it, but that distinction dictates everything we do next.
Ignoring the Whisper: Elias’s Urgent Lesson on Listening to Pain
I remember meeting a patient named Elias about two years ago. He was a 58-year-old carpenter, a tough guy who never complained. He came into the clinic clutching his left side, looking pale. He told me he’d been feeling “off” for weeks, just a little twinge here and there, but he ignored it. He kept working, lifting heavy lumber, thinking it was a pulled muscle. By the time he saw me, he had a high fever and couldn’t stand straight. Elias taught me that this condition loves to whisper before it screams. He ignored the whisper, so he had to deal with the scream.
Recognizing the Symptoms
You might be wondering if what you’re feeling is actually Diverticulitis or just a bad stomach ache. While I can’t diagnose you through a screen, there is a very specific pattern we look for here at Medical4Me.
Here is what typically happens:
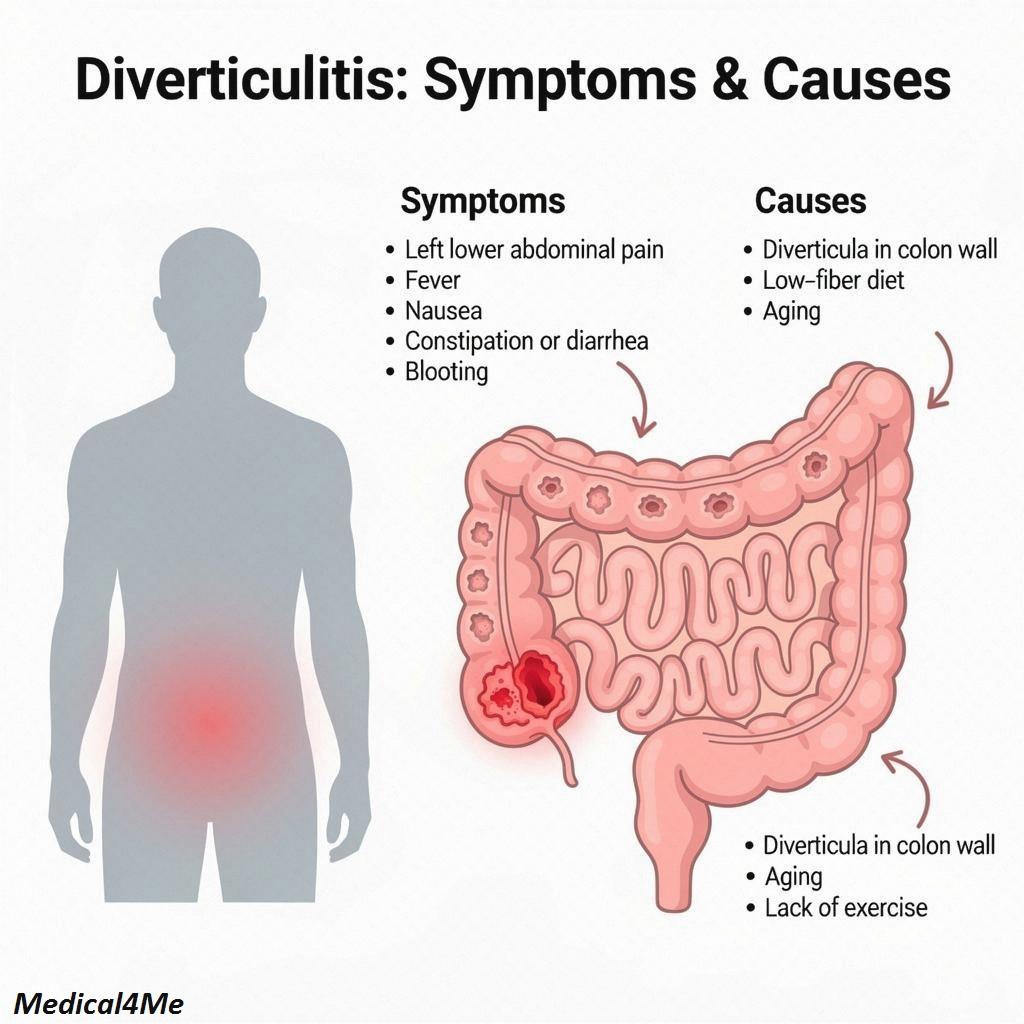
- The “Left-Sided” Pain: This is the hallmark. In Western populations, the pain is almost always in the lower left side of your abdomen (LLQ). It can start mild and ramp up over days.
- Fever and Chills: Because this is an infection, your body heats up to fight it.
- Nausea and Vomiting: Your gut is unhappy and wants to stop processing food.
- Change in Bowel Habits: You might suddenly be constipated or, conversely, have diarrhea.
- Abdominal Tenderness: If you press on that spot on your left side and it hurts more when you let go (rebound tenderness), that’s a sign you need help.
If you have these, especially the fever combined with the pain, it’s time to see a professional.
Root Causes and Risk Factors
Why does this happen? It’s usually a combination of pressure and weakness. If you strain too hard on the toilet often (chronic constipation), you are increasing the pressure inside that “tire” (your colon). Over years, this pushes the lining out through weak spots in the muscle wall.
I mentioned in recent posts that age is the biggest factor. But it’s not the only one.
The Struggle is Real: Sarah’s Experience with Diverticulitis
This brings me to Sarah. She was only 34, a graphic designer who spent 12 hours a day sitting at a desk. She was shocked when I told her she had Diverticulitis. “Isn’t that an old person’s disease?” she asked me, terrified. Sarah lived on fast food and coffee—very little fiber, lots of processed sugar. Her lifestyle had created a high-pressure environment in her colon despite her youth. She shows us that this isn’t just about age; it’s about how we treat our insides.
The Diagnostic Journey
If you come to see a doctor, you shouldn’t worry about the process. It is straightforward. Here is exactly what I would do if you were sitting in my clinic right now:
- The Physical Exam: I would gently press on your abdomen to feel for tenderness or a mass. I’d listen to your bowel sounds.
- Blood and Urine Tests: We need to check your white blood cell count. If it’s high, it confirms an infection. We also check urine to rule out a kidney infection, which can feel similar.
- The CT Scan: This is the gold standard. As Mayo Clinic explains, a CT scan lets us see the pockets, the inflammation, and if there are any complications like an abscess.
- Stool Test: Sometimes needed to rule out other bugs.
Treatment Reality
This is the part where you can relax a little. Most people do not need surgery. In fact, the vast majority recover with rest and medication.
Lifestyle Shifts
The immediate “prescription” isn’t a pill; it’s a pause. We need to put your bowel on “bowel rest.” This usually means a clear liquid diet for a few days—broth, water, gelatin. No solid food. This gives the angry tire bubble time to calm down without having to work to move food along.
Medical Options
When we do need to use medication, we reach for antibiotics to kill the bacteria causing the infection. However, NIDDK guidelines suggest that for mild cases, we are prescribing them less often now, but for moderate cases, they are essential.
Here are the real medications I typically prescribe:
- Ciprofloxacin (Cipro): This is a heavy hitter. It works by stopping bacteria from reproducing (it interferes with their DNA).
- Side Effects: It can cause tendon pain or nausea.
- Metronidazole (Flagyl): We often pair this with Cipro. It targets anaerobic bacteria (bugs that live without oxygen) which love the gut.
- Side Effects: It leaves a metallic taste in your mouth and you absolutely cannot drink alcohol with it, or you will get violently ill.
- Amoxicillin-Clavulanate (Augmentin): Sometimes we use this single pill instead of the combo above. It breaks down the bacteria’s cell walls.
- Side Effects: Diarrhea is very common with this one.
Let’s weigh your options.
| Feature | Antibiotics & Rest | Surgery (Resection) |
|---|---|---|
| Recovery Time | Fast (days to a week) | Slow (weeks to months) |
| Invasiveness | Low (just pills) | High (hospital stay) |
| Risk | Side effects like nausea | Infection, recovery complications |
| Permanence | Treats current flare-up only | Removes the problem area permanently |
| Best For | 85% of first-time patients | Recurring, complicated, or severe cases |

When Pills Failed: Martha’s Peace Found Through Surgical Intervention
I’ll never forget Martha, a 72-year-old librarian. She had recurring attacks—three in one year. The antibiotics worked, but the infection kept coming back because that one section of her colon was just too damaged. We finally decided on surgery to remove that small section. She was terrified of the hospital. But afterward? She told me she hadn’t realized how much constant, low-grade pain she had been living in until it was gone. Sometimes, the harder path leads to the best peace.
Red Flags: When to Call 911
I don’t want to scare you, but I need you to be safe. Just like with other conditions involving infection, things can turn quickly. You need to go to the Emergency Room if:
- You have a fever above 100.4 F (38 C) that won’t go down.
- The pain is so severe you can’t stand up.
- You see bright red blood in your stool (a lot of it).
- You feel dizzy, lightheaded, or faint.
Frequently Asked Questions My Patients Ask
Yes. The old advice to avoid nuts and seeds is outdated. Unless you notice they specifically trigger pain for you, they are generally safe.
Indirectly, yes. Stress affects digestion and can lead to spasms in the colon, which might aggravate the condition.
It might. About 20-30% of people have a recurrence. But a high-fiber diet (after you heal) lowers this risk significantly.
No. Diverticulitis is benign. However, because symptoms can overlap, we often do a colonoscopy after you heal just to be sure.
With antibiotics and rest, you should feel significantly better within 2 to 3 days. If you don’t, call your doctor.
Please don’t rely solely on herbs for an active infection. While tea soothes, a perforated colon is life-threatening. Use modern medicine to heal, and herbs to maintain.
My Final Professional Advice
Listen, I know the word “infection” inside your body sounds alarming. But Diverticulitis is something we see, treat, and manage every single day. It is not a mystery to us.
If you are in pain right now, stick to clear liquids. Rest. Don’t try to be a hero like Elias and push through it. Your body is asking for a break, so give it one. And once this passes—and it will pass—we can talk about adding more fiber to your diet and drinking more water to keep those “tires” in good shape.
You are going to be okay. Try to get some sleep now. I’m rooting for you.

Medically Reviewed By
Dr. Saqlain Mushtaq, MBBS
Lead Medical Author, Medical4Me.com
About Our Editorial Process
💬 Share Your Experience
Share your thoughts, questions, or personal tips below. Our community and editorial team value respectful and insightful discussions.