Understanding Osteoporosis
It’s late, and I can imagine you’re sitting there with a cup of tea that’s gone cold, scrolling through terrifying statistics on your phone. Put the phone down for a second. Take a deep breath. I’m Dr. Saqlain Mushtaq, and I want to talk to you not just as a doctor, but as a friend who happens to know a lot about bones.
We are going to walk through this together.
I’ve seen the look in your eyes a thousand times. It’s the fear that your body—the sturdy vessel that has carried you through decades of work, joy, and stress—is suddenly fragile. You hear the word Osteoporosis, and you picture brittle glass. But that isn’t the whole story. Not even close.
Let me tell you about Rashid.
Rashid is 68, a retired accountant. He’s the kind of man who never missed a day of work and still does his own taxes. He came to me thinking he had pulled a muscle while shoveling snow. He wasn’t in agony, just a nagging back pain that wouldn’t quit. We did an X-ray, and there it was: a compression fracture in his spine. He hadn’t fallen. He hadn’t been in a car crash. His bones had simply become too porous to hold up the weight of his own daily life.
Rashid was terrified he’d never lift his grandkids again. But today? He’s back to gardening. He’s careful, yes, but he’s strong. We caught it, we treated it, and he’s living a full life. That can be your story, too.
What Osteoporosis Really Is
To understand this, I need you to forget the medical diagrams for a moment.
Think of your skeleton as a busy construction site. You have two teams working on this site 24/7.
Team A (The Demolition Crew) clears out old, damaged bone.
Team B (The Builders) lays down fresh, strong new bone.
For the first 30 years of your life, the Builders are faster. They are overachievers, packing density into your frame like money in a high-yield savings account. But as we age—and especially after menopause for women—the Demolition Crew starts working overtime, and the Builders get a bit lazy. They can’t keep up.
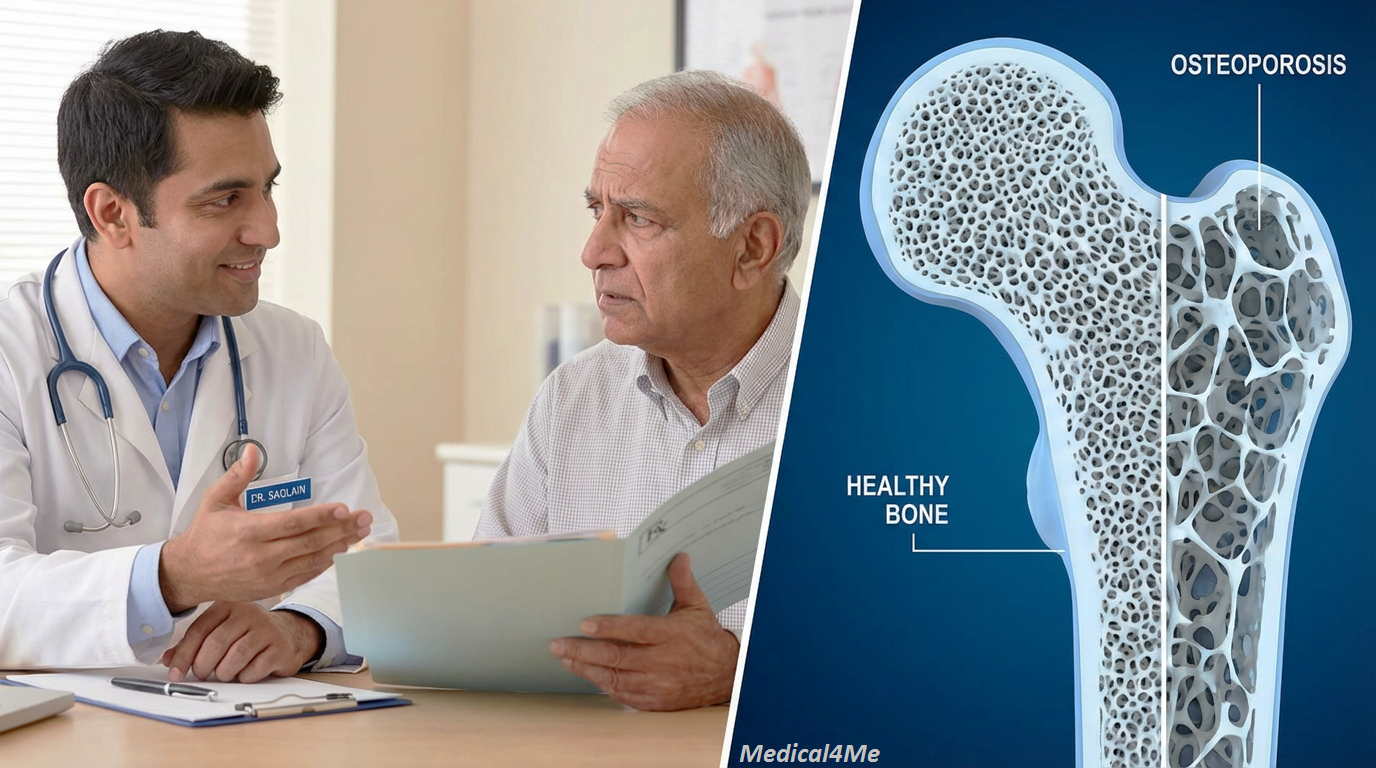
Osteoporosis happens when the Demolition Crew has removed so much material that the scaffolding of your “house” gets thin. It’s not that your bones are dead; it’s that the renovation project has fallen behind schedule.
My first thought when a patient describes this diagnosis is always, “Okay, the balance is off. How do we fire the demolition crew and hire more builders?” It’s a management problem, and we can manage it.
Recognizing the Symptoms
This is the tricky part. I often call this the “Silent Thief” because it steals your bone density without you feeling a thing. You don’t feel your bones getting thinner any more than you feel your hair growing.
However, there are signs if you look closely. Here is what I want you to watch for:
- Receding Gums: Surprisingly, your jawbone can lose density first, causing gums to pull back.
- Weaker Grip Strength: There is a weirdly strong correlation between how hard you can squeeze a handle and the density of your hips and spine.
- Height Loss: If you notice you are an inch shorter than you were ten years ago, that isn’t just “getting old.” It’s often tiny fractures in the spine compressing.
- Back Pain: Specifically, a nagging, dull ache in the lower back or neck that worsens when you stand.
- The “Fragility” Fracture: This is the big one. If you fall from a standing height (just a trip, not a fall off a ladder) and break a bone, that is a major red flag.
Root Causes
Why does this happen? It’s rarely just one thing.
I remember treating a young woman named Maria, only 34. She was a brilliant architect. She was baffled because she thought this was an “old person’s disease.” But Maria had severe asthma and had been on high-dose steroids (like prednisone) for years. Those lifesaving drugs, unfortunately, are like fuel for that “Demolition Crew” I mentioned.
Common culprits include:
- Estrogen Drop: Hormones protect bone. When they drop during menopause, protection fades.
- Medications: Steroids, some seizure meds, and even some acid reflux drugs can interfere with absorption.
- Nutritional Gaps: If you didn’t get enough calcium and Vitamin D growing up, your “savings account” started low.
- Sedentary Life: Bones get stronger under stress (gravity). If you sit all day, your bones think, “I guess we don’t need to be strong,” and they shed density.
Because of this, we have to look at your whole life, not just your X-rays, just like with other conditions we manage.
The Diagnostic Journey
If you are worried, don’t just guess. Here is the roadmap I use for my patients. It is painless, I promise.
- The Clinical History: We talk. I ask about your parents (genetics are huge here) and your diet.
- The DEXA Scan: This is the gold standard. It’s an X-ray, but very low radiation. You lie on a table, a machine arm passes over you, and it measures exactly how dense your hip and spine are.
- The T-Score: The machine gives us a number.
- 0 to -1: Normal. You’re doing great.
- -1 to -2.5: Osteopenia (Low bone mass, but not quite broken yet).
- -2.5 or lower: Osteoporosis.
- Blood Work: We check calcium, Vitamin D, and thyroid function to rule out other causes.
- The FRAX Score: This calculates your 10-year probability of breaking a hip. It helps us decide if you really need medicine or just a lifestyle overhaul.
To be perfectly honest, the medical community is still exploring the precise mechanism of why some people with “good” scores still fracture, while others with “bad” scores don’t. But these tools are the best maps we have right now.
Treatment Reality
So, you have the diagnosis. Now what? We fight back.
Lifestyle: The Foundation
Before pills, we look at your day-to-day. I had a patient, Ubaid, 72, who loved to read but hated milk. We got him on heavy leafy greens, almonds, and a daily walk. We added weight-bearing exercises—literally lifting heavy things. His bone density didn’t just stabilize; it improved slightly. You need to signal to your body that you need these bones.
Medical Options
Sometimes, salad and walking aren’t enough. That is okay. Science has given us incredible tools.
Common medications I prescribe include:
1. Alendronate (Fosamax):
This belongs to a class called bisphosphonates. Think of this drug as “handcuffs” for the Demolition Crew. It stops the cells that break down bone from working so fast.
How it works: It binds to the bone surface and slows resorption.
Side Effects: It can cause heartburn or esophageal irritation. You have to stay upright for 30 minutes after taking it.
2. Denosumab (Prolia):
This is an injection given every six months. It’s a bit more advanced. It blocks the chemical signal that calls the Demolition Crew to the site in the first place.
How it works: It’s an antibody that targets the RANK ligand (the signal).
Side Effects: Back pain, and a slight risk of skin infections.

Comparing Your Paths:
| Feature | Lifestyle Only | Medication + Lifestyle |
|---|---|---|
| Speed of Effect | Slow (Years) | Moderate to Fast (Months) |
| Side Effects | None (actually improves overall health) | Possible (Digestive issues, muscle pain) |
| Bone Density Change | Maintains current density | Can actively increase density |
| Best For | Prevention / Osteopenia | Established Osteoporosis |
The Mayo Clinic explains that medication choice depends heavily on your personal history, which is why we tailor this.
Warning Signs
While we can manage this, there are moments you need to act fast. Call me or go to urgent care if:
- You have sudden, severe back pain that limits movement.
- You notice one hip looks higher than the other.
- You fall and cannot get up, or there is immediate swelling/deformity in a limb.
Frequently Asked Questions My Patients Ask
You can stop it from getting worse, and maybe improve it slightly, but fully “reversing” it usually requires medication alongside lifestyle changes.
Yes! In fact, it is dangerous not to. We just need to avoid high-impact jumping or deep twisting of the spine.
Absolutely. About 20% of osteoporosis patients are men. They just tend to get diagnosed later, which makes it riskier.
It helps, but milk alone isn’t magic. You need Vitamin D to actually absorb that calcium. Without D, the milk is just passing through.
Not necessarily. We often do a “drug holiday” after 3-5 years to reassess, as mentioned in my recent posts.
My Final Professional Advice
I want to leave you with one last story.
I treat a woman named Anita. She is from Lahore originally, but has lived in New York for forty years. She was diagnosed with severe osteoporosis at 65. She was scared to pick up her cat. She felt like her body had betrayed her.
We started treatment. She took up Tai Chi for balance. She took her calcium. Last week, at 70, she showed me photos of her hiking trip in the Rockies. She wasn’t running up the mountain, but she was climbing it, steady and sure.
Osteoporosis is a warning sign, not a stop sign. It is your body asking for a little more support. Listen to it. Take your meds if you need them. Eat your greens. Walk in the sunshine.
You are not made of glass. You are made of living, changing tissue that can heal. You’ve got this, and if you get stuck, I’m right here.
Now, finish that tea and get some sleep. Your bones need the rest.

Medically Reviewed By
Dr. Saqlain Mushtaq, MBBS
Lead Medical Author, Medical4Me.com
About Our Editorial Process
💬 Share Your Experience
Share your thoughts, questions, or personal tips below. Our community and editorial team value respectful and insightful discussions.